02xl is your source for accurate and trustworthy information so you can make the best choices for your health and wellness.
PS: Please note that 02xl provides this information for the benefit of the rare disease and overweight community. 02xl is not a medical provider or health care facility and thus can neither diagnose any disease or disorder nor endorse or recommend any specific medical treatments. Patients must rely on the personal and individualized medical advice of their qualified health care professionals before seeking any information related to their particular diagnosis, cure or treatment of a condition or disorder.
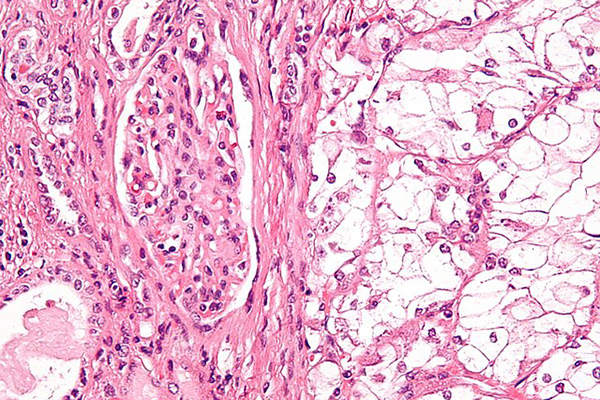
For clinicians who treat patients with renal cell carcinoma (RCC), the PDQ Cancer Genetics Editorial Board has recently updated peer-reviewed, evidence-based information regarding the genetics of RCC.1
RCC, the most common type of kidney cancer, refers to tumors that develop in the kidney parenchyma, including the renal tubules. RCC contributes to approximately 4% of adult malignancies and in 2017, alone 63,990 cases are estimated to have occurred, leading to more than 14,400 deaths.

RCC can be sporadic or heritable, with approximately 5% to 8% of RCC cases attributed to pathogenic germline variants that are inherited in an autosomal dominant pattern. To date, four major RCC syndromes have been identified that exhibit an autosomal dominant inheritance pattern, including hereditary papillary renal carcinoma (HPRC; caused by pathogenic variants in MET), von Hippel-Lindau disease (VHL; caused by pathogenic variants in VHL), Birt-Hogg-Dubé syndrome (BHD; caused by pathogenic variants in FLCN), and hereditary leiomyomatosis and renal cell cancer (HLRCC; caused by pathogenic variants in FH). With the exception of HPRC, these syndromes are associated with other tumors in other organs.
This PDQ cancer information summary was last updated online November 21, 2017 by the PDQ Cancer Genetics Editorial Board, which is independent of the National Cancer Institute. The purpose of this summary is to provide a resource for clinicians caring for cancer patients. No formal recommendations or guidelines are provided.
Family history as a risk factor
“My inspiration,” Michael Hall, MD, MS, Associate Professor, Department of Clinical Genetics, Fox Chase Cancer Center, Philadelphia, Pennsylvania, told MedPage Today, “comes from a few places. I come from a family with many cancers, so, certainly some of my inspiration comes from wanting to understand better how diseases like cancer occur in families and how we can do a better job preventing them.”
Population-based registry studies support the idea that a family history of RCC is a risk factor for developing RCC ..2,3,4 Hereditary RCC cancers are often diagnosed earlier than the fifth to seventh decades of life, in contrast with sporadic cases of RCC. An NCI review reported that 70% of the 600 cases of hereditary cancer cases were diagnosed ≤46 years of age. Currently, no consensus exists regarding referral for genetic testing for hereditary kidney cancer syndromes.
Hereditary papillary renal carcinoma (HPRC)
Individuals with HPRC are predisposed to developing bilateral and multifocal type 1 papillary RCC. Major risk factors for HPRC include a relative with bilateral multifocal type 1 papillary RCC and/or an activating pathogenic variant in the tyrosine kinase domain of the MET proto-oncogene. Currently, all reported cases of HPRC have presented with type 1 papillary RCC. No extra-renal manifestations have been reported.
Genetic testing is available and recommended if an individual has at least one of the following: 1) a family history of HPRC; 2) a biological relative with a positive genetic test result for a pathogenic variant in the tyrosine kinase domain of MET; 3) >1 papillary type 1 RCC, a papillary type 1 RCC with lesions of the surrounding parenchyma, or a papillary type 1 RCC diagnosed at younger than 45 years of age.
Von Hippel-Lindau disease (VHL)
VHL is a tumor suppressor gene, with pathogenic variants occurring in each of the 3 exons. Affected individuals inherit a germline pathogenic variant and a wild-type copy of the VHL gene, which requires damage to the wild-type allele to result in cancer progression. VHL is frequently diagnosed in patients with no family history of VHL, which comprises about 23% of affected individuals. Approximately 1 in 35,000 to 40,000 people have VHL, with an estimated 6000-7000 VHL-affected Americans.
Patients with VHL variants are predisposed to central nervous system hemangioblastomas; retinal angiomas; renal cysts and clear cell RCCs; cysts, cystadenomas, pheochromocytomas, and neuroendocrine tumors of the pancreas; cystadenomas of the epididymis (men) and of the broad ligament (women); and endolymphatic sac tumors.2-4 The updated PDQ guidelines recommend multidisciplinary evaluation and management of patients with VHL.
Type I VHL is associated with large gene deletions and the development of VHL-associated lesions except pheochromocytoma. Type II VHL is more frequently associated with missense variants and the development of all VHL-associated lesions.
Onset of VHL can be seen at varying ages among families and between members of the same family. Targeted screening for retinal hemangioblastomas and pheochromocytomas is recommended in children younger than 10 years of age.
Birt-Hogg-Dubé syndrome (BHD)
BHD is a rare autosomal dominant disease that results from mutations in the FLCN (folliculin) gene. Over 200 families affected with BHD from various populations in the US, UK, Australia, Canada, Denmark, Italy, Japan, Spain, and the Netherlands have been reported. The syndrome is characterized by skin and lung manifestations including and increased risks of of renal tumors, and pulmonary cysts/history of spontaneous pneumothorax. The characteristic skin findings include fibrofolliculomas, noncancerous tumors that can appear on the face, neck, and chest. An estimated 15% to 30% of individuals with BHD develop renal tumors at a median age of 46 to 50 years. These tumors are bilateral, slow-growing, and multifocal, with approximately 50% hybrid oncocytic tumors, 34% chromophobe RCC, and 9% oncocytomas.
Genetic testing is recommended for individuals with the following: 1) ≥5 facial or truncal papules and ≥1 histologically confirmed fibrofolliculoma with or without BHD family history; 2) BHD family history with a single fibrofolliculoma or renal tumor or history of spontaneous pneumothorax; 3) multiple and bilateral chromophobe and/or oncocytic hybrid renal tumors; 4) a single chromophobe or oncocytic hybrid tumor and a family history of any renal cancer; 5) a family history of autosomal dominant primary spontaneous pneumothorax with no history of lung cyst.
Hereditary leiomyomatosis and renal cell cancer (HLRCC)
HLRCC is characterized by cutaneous leiomyomas, RCC, and/or uterine leiomyomas (fibroids) in women. Although HLRCC prevalence is unknown, several hundred families have been evaluated at the NIH and other centers globally, with the thought that HLRCC continues to be under-ecognized.
Inheriting a single FH (fumarate hydratase) variant allele predisposes an individual to develop disease manifestations. If two pathogenic variants are inherited, an individual develops FH deficiency, which is characterized by neurologic impairment that rapidly progresses, including seizures, hypotonia, and cerebral atrophy. No correlation has been reported between variants of FH and the development of RCC, cutaneous lesions, or uterine leiomyomas.
Genetic testing is available for FH, which is currently the only known gene to be associated with HLRCC. Genetic testing can be used to identify at-risk family members earlier, reducing costly and stressful screening procedures in family members without the pathogenic variant.
There is no consensus regarding clinical surveillance; however, individuals with heterozygous pathogenic FH variants and at-risk family members that have not undergone genetic testing should be followed regularly.
Conclusion
In this summary, the PDQ Cancer Genetics Editorial Board provide information related to the four major hereditary RCC syndromes, including HPRC, VHL, BHD, and HLRCC. No formal guidelines or recommendations are provided in this publication, but published peer-reviewed articles are discussed , providing guidance to clinicians on screening based on family history, clinical suspicion, and other factors.
Published:



